
Does erythritol increase the risk of heart disease?
Written by Robb Wolf (opens in a new tab)
<p>In February of 2023, researchers published a <a href="https://www.nature.com/articles/s41591-023-02223-9." rel="noopener noreferrer" target="_blank">now-famous paper</a> about the dangers of erythritol—a popular low-carb sweetener—in the prestigious branch of <em>Nature</em>, <em>Nature Medicine</em>.<em> </em>The findings suggest that consuming erythritol may increase one’s risk of blood clots and adverse cardiac events.</p><p>The authors present several lines of evidence—observational, mechanistic, and clinical—that make me a bit wary about erythritol. I rarely eat keto sweets, so I’m not making drastic changes in my<em> </em>diet, but I think people who substitute erythritol for sugar should know what the study says to make informed decisions about their own health.</p><p>Many people eat keto desserts, and the amount of erythritol in a pint of keto ice cream is about the same dose used (from the study) to elevate serum erythritol levels “well above the thresholds necessary to enhance stimulus-dependent platelet reactivity” (aka, clotting risk) in a group of healthy people. It’s also concerning that erythritol levels stayed significantly elevated for two days or more post-ingestion, which is a relatively long time to sustain elevated clotting risk. I’ll return to this data later.</p><p>My goal today is to review the findings in a balanced<em> </em>way. I don’t believe we should dismiss this data—and I’m not ignoring the potential link to heart issues—but we should also take our time and be thoughtful in our analysis. It’s a bit early to start campaigning for a Prohibition-style ban on erythritol.</p><p>Let’s begin with the first finding: The observational data.</p><h2><strong>Erythritol Levels and Cardiac Events (Observational Data)</strong></h2><p>As a first step, the researchers screened 1,157 people for the presence of various molecules in their systems (including erythritol) and the incidence of major adverse cardiac events (MACE) over 3 years. After finding a link between erythritol and MACE, researchers moved to the “validation cohorts.”</p><p>The authors then assessed erythritol levels in these cohorts (about 3,000 people from the US and Europe). They found that:</p><ol><li>Participants with higher erythritol levels were more likely to have existing cardiovascular disease (CVD)</li><li>Over the next 3 years, people with higher erythritol levels experienced more cardiac events</li></ol><p>Of course, this is correlational data and doesn’t prove causation. But any old monkey like myself can say that, so let’s dig deeper and ask more questions.</p><h3><strong>Questions and Confounders</strong></h3><p>Mammals produce erythritol endogenously via the pentose-phosphate pathway, and—here’s the confounder—metabolically dysfunctional mammals <a href="https://pubmed.ncbi.nlm.nih.gov/32412980/" rel="noopener noreferrer" target="_blank">produce <em>more </em>erythritol</a>. In other words, sick mammals, people included, produce more erythritol. Were higher erythritol levels <em>the cause</em> of increased CVD risk of subjects in the study, or was elevated serum erythritol <em>a symptom</em> of metabolic issues that separately influenced their CVD risk? The observational data can’t answer that question.</p><p>Drawing firm conclusions here is hairy because <em>many</em> factors influence the <a href="https://pubmed.ncbi.nlm.nih.gov/17456293/" rel="noopener noreferrer" target="_blank">relationship</a> between metabolic syndrome and CVD. For starters, high blood glucose, high blood pressure, and inflammation all increase CVD risk. You also have the usual confounders—poor sleep, sedentary lifestyle, nutrient deficiencies—that accompany metabolic disorders. I don’t care what fancy stats you use; you can’t “adjust” for every lifestyle factor. There are simply too many.</p><p>One last point is that the validation cohorts (primarily folks in their 60s and 70s) were pretty high-risk from the outset. About 1 quarter of them had diabetes. Between 70 to 80 percent had hypertension. Almost half had a prior heart attack. Data from this population might not track well with data from healthier populations.</p><h2><strong>Erythritol and Clotting (Mechanistic Data)</strong></h2><p>Next, we proceed to data suggesting that higher erythritol levels increase platelet aggregation, aka clotting risk. If this is true, we may have a plausible mechanism by which this sweetener affects CVD risk. Clots that form in the arteries can break off to cause heart attacks, strokes, or sudden death.</p><p>To test the clotting hypothesis, the researchers combined human platelet-rich plasma (PRP) and whole blood with erythritol <em>in vitro</em> (in a test tube or culture dish). “We were careful,” note the authors, “to use erythritol concentrations within the range observed among the fasting samples examined in subjects from the US and European validation cohorts.” They found that erythritol increased platelet aggregation in a dose-dependent manner. Higher erythritol levels appear to cause platelets to release more calcium, driving thrombosis (clotting). They also found that erythritol increased thrombosis in mice.</p><h3><strong>Questions and Confounders</strong></h3><p>First, I’d love to see researchers create a coagulation panel—a screening test for abnormal blood clotting—for erythritol specifically. (<a href="https://www.ncbi.nlm.nih.gov/pmc/?term=erythritol+coagulation" rel="noopener noreferrer" target="_blank">Nobody has</a>, as far as I can tell.) It’s an easy test and would be more convincing than the in vitro data described above.</p><p>Another wrinkle in the above data involves glucose. The authors found that while higher levels of erythritol increased clotting risk (in test tube PRP), <a href="https://www.nature.com/articles/s41591-023-02223-9/figures/10" rel="noopener noreferrer" target="_blank">normal levels</a> of glucose did not. This seems an odd comparison since we already understand that normal glucose levels don’t cause clotting. But animal evidence suggests that higher glucose levels (hyperglycemia) <em>do </em><a href="https://diabetesjournals.org/diabetes/article/68/5/932/39738/Glucose-Metabolism-Is-Required-for-Platelet#" rel="noopener noreferrer" target="_blank">increase</a> platelet aggregation.</p><p>My point? Many folks from the observational data had high glucose levels. So the question is, was it high erythritol levels or high glucose levels that influenced thrombosis and CVD risk? Perhaps it was both.</p><h2><strong>Erythritol Ingestion in Healthy People (Clinical Data)</strong></h2><p>The final experiment is probably the most concerning. It suggests that consuming <em>reasonable </em>doses of erythritol boosts clotting risk <em>for days</em>. Let’s review the experiment design.</p><p>The researchers fed 8 healthy people 30 grams of erythritol (about what’s in a pint of keto ice cream), then measured subjects’ blood erythritol levels at future times. At 30 minutes, their erythritol levels were up nearly 1000x from baseline. At 2 days, levels were still high enough to correspond with increased thrombosis risk.</p><h3><strong>Questions and Confounders</strong></h3><p>Some people dismiss this experiment because it only had 8 participants. <em>The n is too small to draw meaningful conclusions, no? </em></p><p>I don’t see it this way. Notice the immense<em>, </em>consistent spike in erythritol levels in all 8 participants from the figure below. Also, notice the consistency of the time to clear it. (Erythritol is excreted via urine, not metabolized like other compounds, which likely explains the slow clearance.) It’s NOT a subtle effect requiring large numbers to detect.</p>
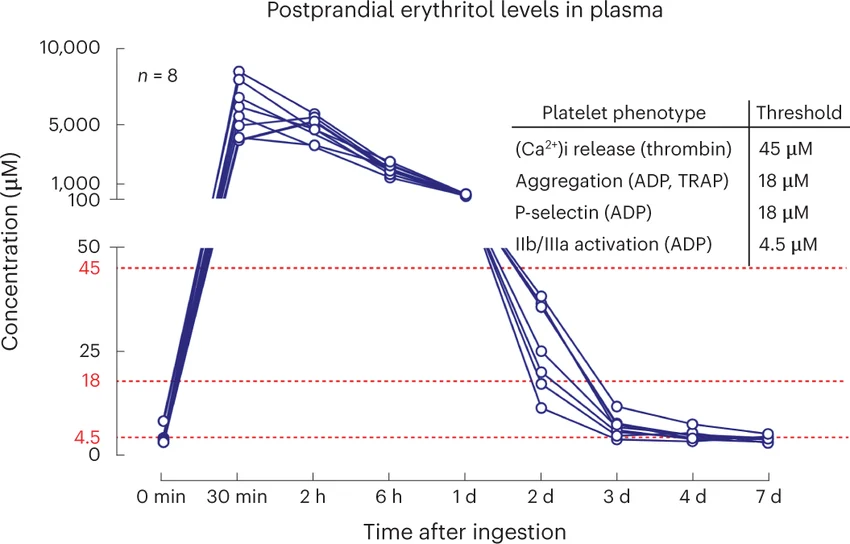
<p>But I do wonder about a <a href="https://www.ahajournals.org/doi/10.1161/atvb.33.suppl_1.A359" rel="noopener noreferrer" target="_blank">2018 pilot study</a> that suggested similar dosages of erythritol <em>improved </em>vascular function in 24 people with type 2 diabetes 2 hours after ingestion AND 28 days later with daily dosing. This study wasn’t looking at clotting specifically, but it seems misaligned with the <em>Nature Medicine </em>results. Did the antioxidant properties of erythritol offset its thrombotic effects? Was it something else? Science doesn’t have answers yet.</p><h2><strong>Thinking Rationally About Erythritol</strong></h2><p><strong>So does erythritol increase the risk of cardiovascular disease?</strong> It’s possible, but it seems a bit soon to stand outside your local supermarket twirling an “Erythritol Is Murder” poster while staring down confused strangers.</p><p>As comprehensive as their research was, the researchers could have done something remarkably simple to answer our question: Conduct a double blind study in which one group is fed some quantity of erythritol, and a control group is not. Then, assess both groups via a <a href="https://www.aacc.org/cln/articles/2012/january/coagulation-tests" rel="noopener noreferrer" target="_blank">coagulation panel</a> to determine if erythritol is indeed dangerous.</p><p>Why would researchers neglect to conduct this simple and effective test? Maybe I need to start buying tin foil by the ream, but it seems fishy to me. You may certainly dismiss all this, but <a href="https://jamanetwork.com/journals/jamainternalmedicine/article-abstract/2548255" rel="noopener noreferrer" target="_blank">big sugar does not have a great track record</a> when it comes to honesty and transparency.</p><p>Despite my misgivings, I also don’t recommend ignoring the <em>Nature Medicine </em><a href="https://www.nature.com/articles/s41591-023-02223-9." rel="noopener noreferrer" target="_blank">study</a>. It provided multiple lines of evidence that erythritol consumption may drive unfavorable cardiovascular outcomes. None of that evidence is a slam dunk—and confounders abound—but nonetheless, it’s worth keeping an eye on. That’s the nice thing about honest, transparent scientific inquiry: With rigorous scrutiny, the truth is made clear and BS eventually makes itself known.</p>